How to Build a Virtual Nurse App Like Sensely? (Cost, Features & Process)
Building a virtual nurse app like Sensely requires a lot more than coding. This guide walks you through development approaches, key features, a step-by-step process, and realistic costs to help startups and healthcare brands launch a trusted, scalable digital nurse solution.
Summarise with AI
- Start small and focused. Don’t try to build another Sensely overnight. Pick one use case and get it right before expanding.
- Bring in the right expertise early. If that’s missing in-house, partner with an experienced agency.
- Budget and build smart. A simple MVP can start around $10K–$70K, while a full-fledged, AI-powered version can go beyond $180K. Build in phases to control cost and risk.
I’ve seen countless healthcare startups come to us with one line: “We want to build something like Sensely.”
And honestly, I get why. Sensely nailed what most health apps miss. A virtual nurse that doesn’t just chat but understands, guides, and escalates intelligently. Behind that simple avatar lies years of clinical validation, workflow mapping, and compliance engineering.
Building something like Sensely isn’t about copying features. It’s about combining AI, healthcare UX, and clinical safety in a way that patients trust and providers approve. Most teams underestimate that balance.
In this guide, I’ll break down how companies actually build virtual nursing software. From choosing the right development approach (in-house, offshore, or through an expert agency) to the step-by-step process, must-have features, and what it realistically costs to get it done.
By the end, you’ll know exactly what to prioritize, what to avoid, and how to turn a “virtual nurse” idea into a working, compliant product that real clinicians would actually use.
Table of Contents
How Do People Build Virtual Nursing Software Like Sensely?
There’s no single “right” way to build a virtual nurse app, but I’ve seen three main approaches work in real projects.
Each works under different goals, budgets, and internal capacities. What matters is picking one that matches your stage, not just what looks good on paper.
1. Building In-House
Some teams try to build everything internally. It makes sense when you’re a well-funded startup or a healthcare provider that wants total control. Including data handling to comply with long-term IP ownership.
But here’s the reality: you’re not just hiring app developers. You’ll need AI engineers, conversation designers, backend architects, healthcare compliance specialists, and clinical advisors. And that hiring cycle can easily stretch your timeline by months.
In-house works best when your virtual nurse is your core product. Something you’ll keep evolving, not a one-time build.
Just note that, if you choose the in-house route, you’ll need to hire app developers, AI engineers, and clinical specialists. This is a process that can take months and stretch your timeline.
2. Hiring Offshore or Hybrid Teams
This is the middle ground. Many of our clients start with a hybrid model, strategy, and design in-house, with development offshore. It’s faster and cheaper than hiring locally, but it only works if you’ve got a strong internal product lead who can manage communication, documentation, and sprint reviews.
You’ll save 30–40% in development cost, but you’ll pay it back in project management and clarity. The key is to set up clear documentation, compliance guidelines, and QA gates early. A dedicated development team works best.
Also, Offshore works beautifully when you already have a validated prototype or an internal PM who owns the roadmap. Otherwise, expect friction.
3. Partnering with a Specialized Agency
For most startups and healthcare brands, this is the most practical route.
Why? Because an experienced app development company already has the HIPAA-ready frameworks, DevOps setup, and compliance playbooks that would take you months to build.
A good agency won’t just code what you describe. They’ll stress-test your idea against real clinical workflows, recommend proven APIs, and build an MVP that can survive scrutiny from both investors and healthcare partners.
This route is ideal when you want to:
- Launch an MVP fast (under 12–16 weeks)
- Validate the concept with pilot users
- Avoid building a full internal tech team too soon
Pro insight: Choose a healthcare app development company that’s actually shipped healthcare products, not just “AI apps.” Sensely-level projects live at the intersection of empathy, accuracy, and compliance. And you can’t fake that experience.
Step-by-Step Process to Build an App Like Sensely
Let’s get one thing straight. You can’t build a Sensely-level product by “just hiring developers.”
Virtual nursing software demands clinical reliability, regulatory compliance, and conversational empathy. These three things don’t come together by accident.
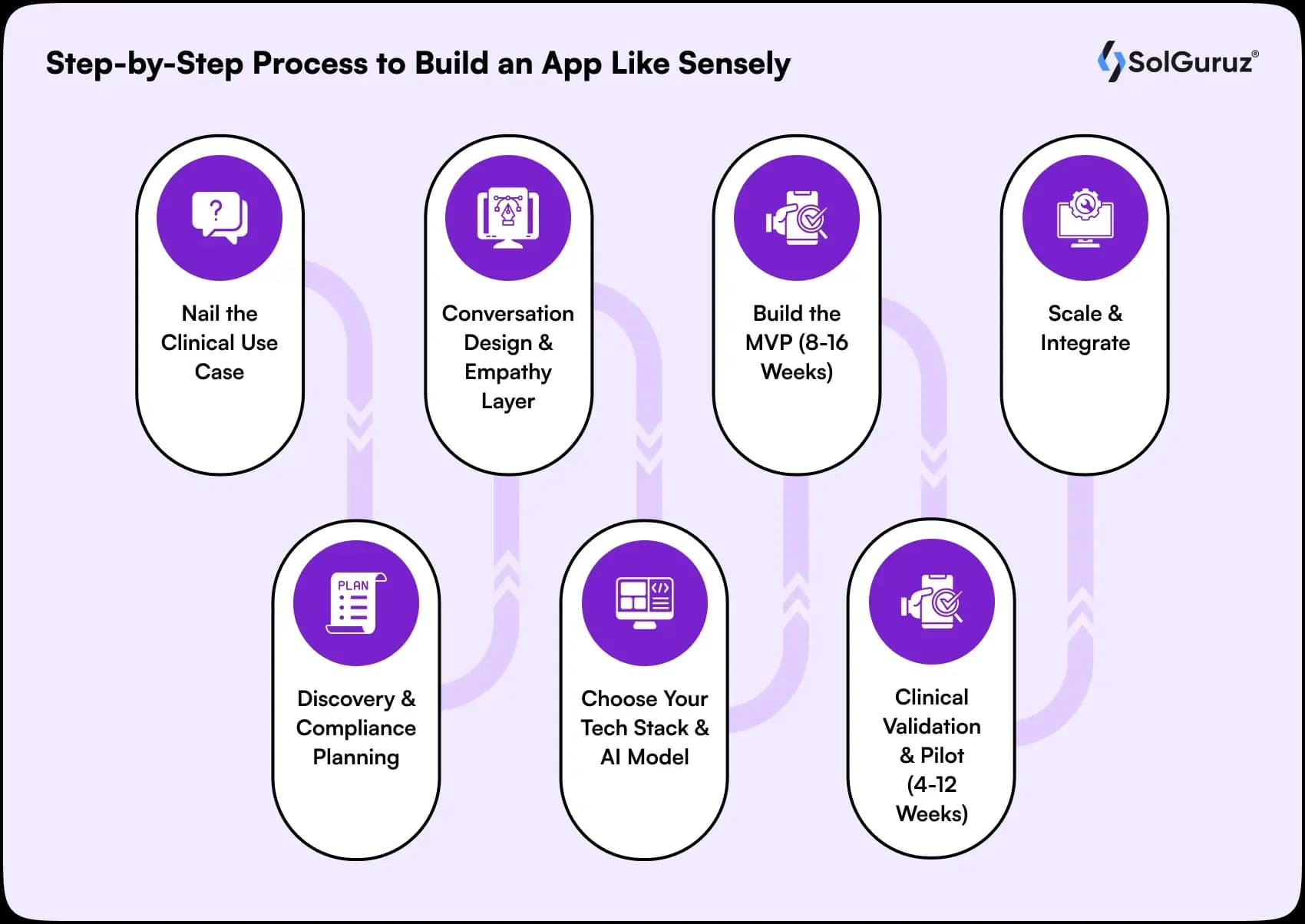
Here’s the actual roadmap we follow when building something like this for clients.
Step 1: Nail the Clinical Use Case
Before touching design or tech, define one clear goal for your virtual nurse:
- Is it for symptom triage?
- Chronic care monitoring (e.g., diabetes, cardiac, post-surgery follow-up)?
- Patient onboarding or insurance navigation?
That single decision changes everything: the compliance scope, the AI design, and even the team composition.
We tell clients this all the time: “The smaller your first use case, the faster you’ll validate it, and the cheaper it’ll be to scale.”
Step 2: Discovery & Compliance Planning
This is where strategy meets regulation.
Our team usually brings in a clinical advisor right from week one. Together, we:
- Map user journeys (patient → virtual nurse → clinician).
- Define escalation rules (what counts as a red flag).
- Plan compliance – HIPAA, GDPR, or local health data laws.
- Identify third-party data sources or APIs you’ll need (EHR, wearables, triage logic).
Skipping compliance planning early is the most expensive mistake founders make. Once your backend is live, retrofitting HIPAA-grade security is not fun (or cheap).
Step 3: Conversation Design & Empathy Layer
Sensely works because it feels human. That’s not AI magic, it’s conversation design.
This stage involves:
- Designing tone, phrasing, and fallback responses.
- Building flows for both structured (menu-based) and free-text inputs.
- Crafting an avatar experience (2D/3D) with inclusive, friendly visuals.
- Designing for accessibility – large fonts, multilingual support, simple UX.
Rule of thumb: If users feel they’re “talking to an app,” you’ve already lost. Your interface needs to listen, respond, and reassure.
Step 4: Choose Your Tech Stack & AI Model
Once the workflows and UX are mapped, pick your tech stack. But don’t over-engineer.
You can start lean with:
Frontend: Flutter or React Native (cross-platform saves cost)
Backend: Node.js or Python (FastAPI/Django)
Database: PostgreSQL or MongoDB (with strict encryption)
AI/NLP:
- Conversational AI: OpenAI, Rasa, or Dialogflow
- Medical triage APIs: Infermedica, HealthTap, or Mediktor
- Speech/Voice: Google Speech or Azure Cognitive
- Avatar: Synthesia, DeepBrain, or custom WebGL model
The smartest MVPs combine off-the-shelf AI + licensed medical engines before attempting custom AI.
Also, check how businesses are using Generative AI in Healthcare.
Step 5: Build an MVP (8–16 Weeks)
Here’s what a working MVP should cover:
- Secure user authentication
- Symptom input and triage response
- Clinician dashboard for escalation
- Conversation logs & analytics
- Feedback loop for clinical review
Avoid overloading your MVP with advanced features like emotion detection or predictive health scoring. At this stage, your only goal is to prove the experience works and the AI doesn’t make unsafe recommendations.
Step 6: Clinical Validation & Pilot (4–12 Weeks)
Once your MVP is live, you’ll run a small pilot. Ideally, with a clinical partner or a small patient group.
During this phase, we measure:
- Triage accuracy (false positives/negatives)
- User engagement (completion rate, satisfaction)
- Escalation effectiveness (how often human review is needed)
The feedback from this stage determines whether you scale or pivot your logic.
If your virtual nurse can’t perform safely under pilot, no hospital or insurer will ever adopt it.
Step 7: Scale & Integrate
Once the pilot succeeds, it’s time to scale.
That’s when we start integrating:
- EHR/EMR (FHIR, HL7)
- Telehealth & scheduling APIs
- Remote patient monitoring (IoT devices)
- Analytics dashboards for clinicians and admins
This is also the stage where you can consider training custom AI models based on anonymized user data. But this comes only after legal and compliance clearance.
Key Features That Actually Make a Virtual Nurse App Work
When clients ask, “Can’t we just add an AI chatbot and symptom checker?”, that’s when I know they’re underestimating what makes Sensely work.
The difference isn’t in the number of features. It’s in how intelligently those features connect to actual healthcare workflows.
Here’s what actually matters:
1. Clinically Reliable Symptom Assessment
This isn’t a glorified chatbot script. It’s a medical decision engine. You’ll need structured triage logic, medical ontologies (like ICD-10 or SNOMED), and continuous validation from medical advisors.
If you skip this, you’ll end up with a “health trivia bot,” not a clinical-grade assistant.
2. Patient-Centric Conversation Layer
Your AI nurse should sound empathetic, not robotic.
We’ve seen teams train models on intent and emotion datasets and use hybrid NLP frameworks (LLMs and rule-based triage) to strike the right balance between conversational warmth and medical accuracy.
That’s what builds patient trust. Not just the avatar.
3. Avatar or Voice Interface (Optional, But Powerful)
Sensely’s avatar isn’t a gimmick; it’s psychology.
Patients open up more to a “face” than a form.
If your audience includes elderly or low-literacy users, investing in a voice or avatar interface genuinely improves engagement metrics.
We’ve built these using Unity frontends with a voice layer from Azure Cognitive Services or AWS Polly.
4. Data Integrations That Don’t Break Things
This is where most projects fail.
Your app must sync with EHR systems, telemedicine platforms, and pharmacy APIs securely, without breaking compliance.
If you’re not using FHIR standards for healthcare data, integration will become your biggest nightmare six months in.
5. Follow-Up Logic & Care Continuity
A good virtual nurse doesn’t vanish after triage.
Build automated follow-ups, medication reminders, and recovery check-ins using workflow automation tools or cloud functions.
The real ROI comes when your product supports patients through their entire care cycle.
6. Multilingual, Accessible, and Compliant
Virtual care only works when it’s inclusive.
Your app must support multilingual NLP, text-to-speech, and accessibility standards (WCAG 2.1).
And yes, HIPAA and GDPR compliance aren’t checkboxes. They’re product pillars. Healthcare partners won’t even pilot without it.
Cost to Develop an App Like Sensely
Let’s be clear. Building something like Sensely isn’t a typical “app development” project. You’re not just paying for screens and APIs; you’re investing in AI, medical logic, and compliance-heavy infrastructure.
So instead of throwing a random number, let’s break it down the way we do when scoping projects for healthcare clients.
1. MVP Range (Proof of Concept): $10,000 to $30,000+
This is where startups test the waters.
At this stage, you’re building:
- A conversational AI nurse (text + limited voice)
- Basic symptom checker with medical rules
- Dashboard for patient monitoring
- Secure login + HIPAA-ready backend
You’ll probably skip EHR integrations and advanced avatars for now. The goal is validation.
2. Full-Scale Production App: $30,000 to $180,000+
Once the MVP works, scaling to Sensely’s level means:
- Full-fledged AI engine (multi-condition triage logic)
- Voice/Avatar interfaces
- EHR + telemedicine integration
- Advanced compliance (HIPAA, GDPR, SOC 2)
- Cloud infrastructure that can scale to thousands of daily assessments
You’ll also need ongoing data training, medical content validation, and DevOps, which can easily add another 20–30% annually in maintenance.
3. What Affects the Cost Most
- Team structure: In-house US dev team will cost 3–4x more than an offshore or hybrid team.
- Tech complexity: Adding avatar-based UX or advanced AI modeling raises costs significantly.
- Regulatory setup: Getting your app audited or certified (e.g., ISO 13485, FDA Class II) adds both cost and time.
4. A More Realistic Approach
The smartest clients don’t try to build Sensely in one go. They build in stages.
They start with an MVP that nails patient interaction and compliance, then expand into avatar UX and AI triage intelligence once the product gets traction.
This phased approach keeps development lean while reducing compliance and tech debt risk.
Concept to Pilot: Key Takeaways

It takes a lot of effort to build a virtual nurse app like Sensely.
Why?
Because it’s an amazing combination of AI + clinical insight + compliance.
And if you ask me, the keys to success are:
- Start small, validate fast.
- Embed clinical oversight early.
- Keep compliance always first.
- Use the right team for your stage.
If you approach it in phases properly, you can easily create a product that works as you want it to.
FAQs
1. How long does it take to build an MVP?
From our experience, a focused MVP can be built in 8–16 weeks. This includes discovery, AI conversation design, backend setup, and a small pilot. Full-scale apps with EHR integrations, avatars, and advanced AI take 6–12 months, sometimes longer if regulatory review is involved.
2. Do I really need a clinical advisor?
Yes, absolutely. AI alone cannot replace clinical oversight. Every triage flow and recommendation must be validated by licensed clinicians. Skipping this creates compliance and safety risks that can derail your app.
3. Can an offshore team handle this?
It depends. Offshore or hybrid teams can cut costs significantly, but you need someone internal to manage compliance, clinical logic, and QA. Without strong internal oversight, you risk misaligned development and regulatory gaps.
4. Should my MVP include voice or avatar features?
Not necessarily. We often recommend starting text-first, focusing on triage accuracy and workflow reliability. Voice or avatar interfaces can be added after you validate patient engagement and AI reliability.
5. What regulatory frameworks are essential?
At a minimum, HIPAA is required for US patients, and GDPR is required for EU patients. Depending on the app, certifications like SOC 2 or ISO 13485 may also apply. These aren’t optional; they are prerequisites for adoption by hospitals or insurers.
6. Can I use off-the-shelf AI for triage?
Yes. Many startups use APIs like Infermedica to accelerate development and reduce clinical risk. Custom AI can be added later once the workflow is validated.
From Insight to Action
Insights define intent. Execution defines results. Understand how we deliver with structure, collaborate through partnerships, and how our guidebooks help leaders make better product decisions.
We Can Help You Build a Sensely Like App
Contact our expert team and begin building a clinically safe app today.

Strict NDA

Trusted by Startups & Enterprises Worldwide

Flexible Engagement Models

1 Week Risk-Free Trial
Give us a call now!

+1 (724) 577-7737